American
![]() f
Manual
Medicine
f
Manual
Medicine
|
American
|
Home
Search
Pain referral
Trigger points
Cranial nerve
Spinal nerve
Historical
Signs and Symptoms of Lesions
Squinting; double vision; tilting of head;
conjugate deviation of the eyes; jerky eye movement; lid drop (Ptosis, possible
Horner’s Syndrome); dizziness; limitation of movement; intermittent pupil
dilation and constriction without light stimuli; oscillating vision.
(Horner’s Syndrome: caused by a brain stem
lesion which effects descending sympathetic nerves ipsilateral to lesion
resulting in face flushing with dryness; narrowing of the palpebral
fissure; upper eyelid drooping; lower eyelid elevation; pupil dilates and is
unresponsive to light (positive red eye reflex); with the entire eyeball
retracting or sunken.)
Oculomotor, Trochlear, and Abducens Nerve Test
There are two steps to test Cranial Nerves
III, IV, and VI:
1.
This maneuver monitor’s conjugate eye movement. The practitioner, utilizing
either a finger or an object, such as a pen, from approximately one foot away,
translates the object through at least 8 planes of the individual’s visual
field. With the individual maintaining a fixed head, the practitioner requests
that the individual follow the object with their eyes only. The practitioner is
observing the individual’s ability to follow the object with their gaze.
The practitioner should note the ability of
the individual to maintain their gaze on the object with both eyes through all
ranges. Inability to concentrically follow an object is a crude indicator
of a lazy eye (amblyopia), multiple sclerosis or occasionally attributed to
increased intracranial pressure.
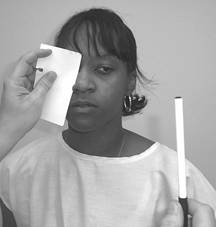
2.
If one eye appears to have the
inability to track the motion of the object, repeat the procedure as listed
above after covering the eye that was able to track the motion.
If the abnormal eye (the one that was unable
to track) is able to track after covering the normal eye, there is a
possibility that there is a problem with the medial and/or longitudinal
fasciculi of the brainstem, which is responsible for conjugate movement.
If the inability to track is not remedied by
covering the normal eye, determine that motion was non-responsive. Loss of downward medial tracking, consider cranial
nerve IV or the superior oblique muscle.
Loss of lateral tracking, consider cranial
nerve VI or the lateral rectus muscle.
With any other deviation, consider cranial
nerve III or extraocular muscles, inferior oblique, medial rectus, superior
rectus and/or inferior rectus. © Copyright
Cranial nerves III, IV, and VI - the Oculomotor, Trochlear, and Abducens nerves

Cranial nerves 3,4, and 6 test 1
Cranial nerves 3, 4, and 6 test 2